Dr C. Covid-19
Name of patient
Disease type

Personal story
Dr C. is a clinical radiologist practicing for more than 25 years in an outpatient care structure with 7 other radiologists.
At the beginning of March 2020 in France, in a few hours, he and his team had to decide whether or not to continue some radiologist activities, reduce their volumes, initially reserve access to imaging services only for patients who absolutely needed it, get equipped (masks, protective clothing, etc.) and train staff in these new ways of working.
His full commitment to the increased activity in the job during this period did not give him time to think that he might one day be infected himself. And yet …
An intense and isolated outbreak of fever woke him up on the night of March 17th (first week of quarantine in France) which prompted him to perform a PCR test on the 18th, which turned out to be negative. Without any other signs, he started to feel tired on the 22nd. A new nocturnal febrile flare-up on the 24th prompted him to do another PCR test on the 25th, which confirmed the diagnosis of Covid-19 on the 26th. His asthenia worsened in a few hours without any respiratory signs. He was forced to be hospitalized that same day noting a severe hypoxia (92 % pulse oximetry). He spent 14 days in the hospital including 4 days in the Intensive Care Unit treated with oxygen therapy/antivirals/antibiotics. He had 2 CT thoracic CT scans during this period, the first one to evaluate on entry the importance of the disease, and the second one with an intravenous contrast injection to exclude, after an acute and nocturne hypotension, the risk of pulmonary embolism. He was discharged on April 8th and was able to return to work at the beginning of May.
Cured, he is now very well.

Radiological Findings
Very quickly and from the beginning of the epidemic the CT chest of patients infected by Sars-Cov-2 (1,2), became essential in the management of this epidemic.
Medical imaging services around the world have very quickly trained their staff to take care of these contagious patients.
Signs on Sars-Cov-2 pneumonitis CT scans are not specific (not sure of the diagnosis) and do not avoid biological sampling to confirm the disease, but it is the easiest way to assess the extent of lung involvement and complications (3).
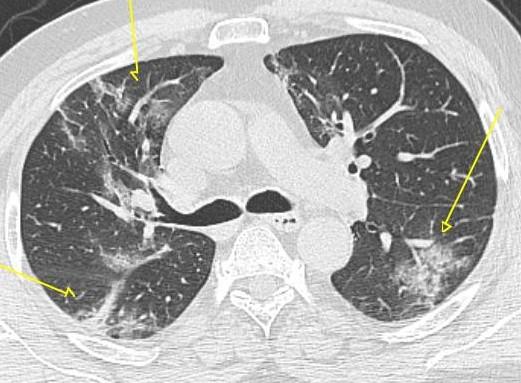
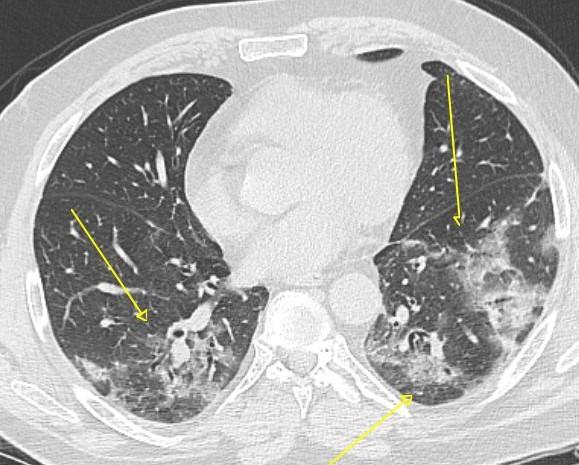
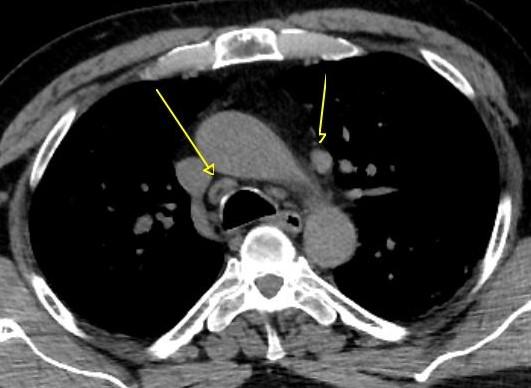
The lungs of patients have ground-glass opacities, peripheral projection, more or less extensive, foci of condensation sometimes more severe (fig.1-2-3 Arrows), reactive lymphadenopathy are found in the mediastinum (nodes reaction to infection)(fig. 4 Arrows). The CT scan makes it possible to quantify the extent of lung involvement at the beginning of management and to look for thromboembolic complications (blood clots in the arteries of the lungs) by injecting an intravenous contrast during the examination. In multi-organ forms (4,5), the CT scan has shown, other than pulmonary (cardiovascular, digestive, renal) and MRI, to be necessary to assess neurological damage.
The chest scan is also the best way to assess the evolution of lung disease during hospitalization and to look for possible fibrous complications (6,7).
References
Bibliography:
- World Health Organization. Pneumonia of unknown caus: China. https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/. Published January 5, 2020. Accessed June 6, 2020.
- M Chung and Coll. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV) Radiology 2020; 295:202–2073.
- TC Kwee and coll. Chest CT in COVID-19: What the Radiologist Needs to Know RadioGraphics 2020; 40:1848–1865
- MV Rezin and coll. Multisystem Imaging Manifesta tions of COVID-19, Part 1: Viral Pathogenesis and Pulmonary and Vascular System Complications RadioGraphics 2020; 40:1574–1599
- MV Rezin and coll. Multisystem Imaging Manifesta tions of COVID-19, Part 2: From Cardiac Complications to Pediatric Manifestations RadioGraphics 2020; 40:1866–1892
- JJ Solomon and Coll. CT of Post-Acute Lung Complications of COVID-19 Radiology 2021; 301:E383–E395
- JP Kanne and Coll. COVID-19 Imaging: What We Know Now and What Remains Unknown Radiology 2021; 299:E262–E279