Mr R. Multiple cancers
Name of patient
Disease type

Personal story
Mr R. is 55-years-old at the beginning of his illness, a former heavy smoker (40 pack-years), married, a father of 2 children and has always been passionate about motorcycling.
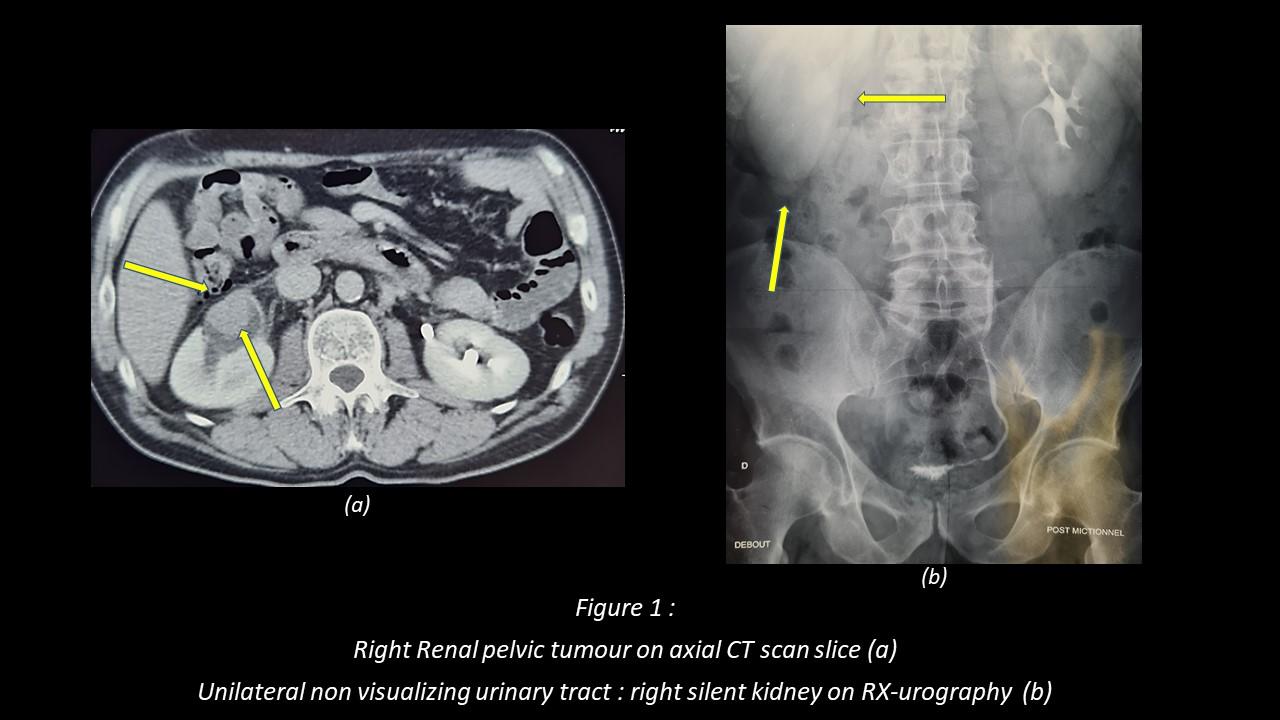
In 2009, just before Christmas, he complained of low back pain, the radiologist who received him for an ultrasound asked to quickly do a CT scan showing a probable right kidney tumour (Figure 1). He was operated on in January 2010 for a malignant urothelial tumour (removal of the kidney, ureter).
Then begins a long radiological follow-up.
In March 2011, a bladder recurrence requires local (cystoscopic) treatment.
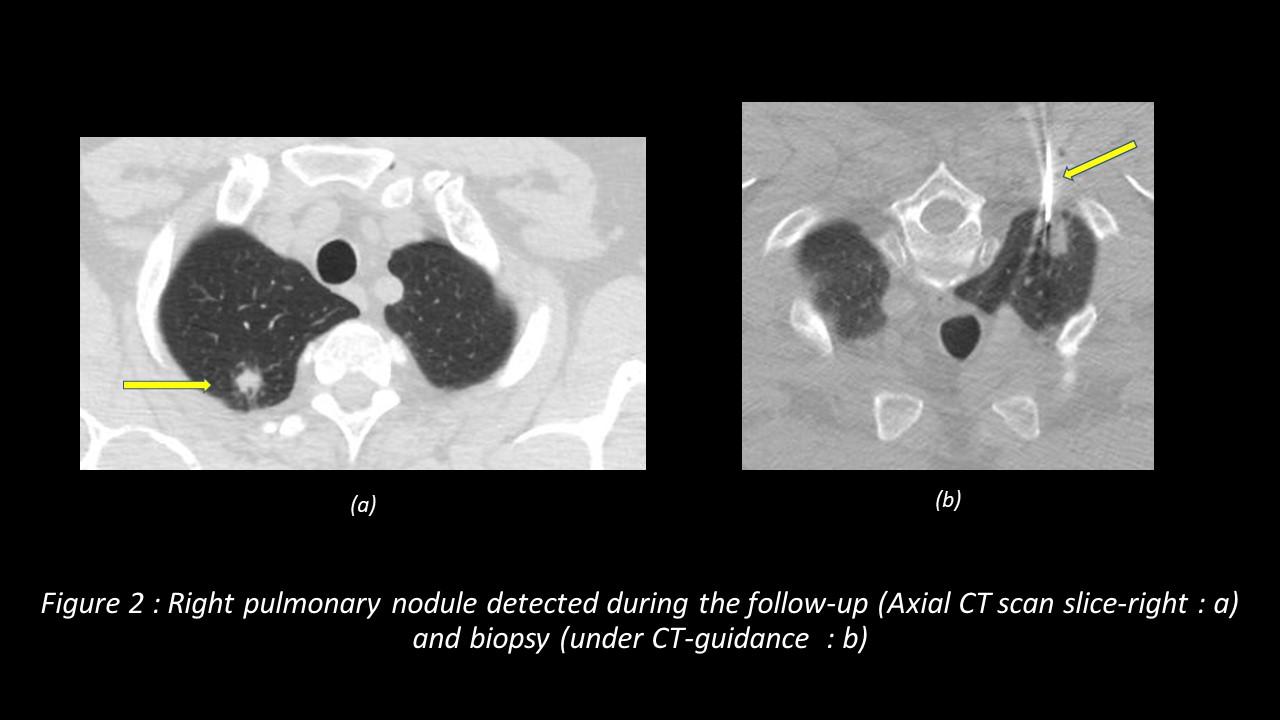
In 2014, a CT follow-up revealed a primary lung cancer (adenocarcinoma) (Figure 2) requiring surgical removal (right superior lobectomy). He was diagnosed few months later with a cancerous polyp (villous adenoma) of the colon (resected simply in colonoscopy).
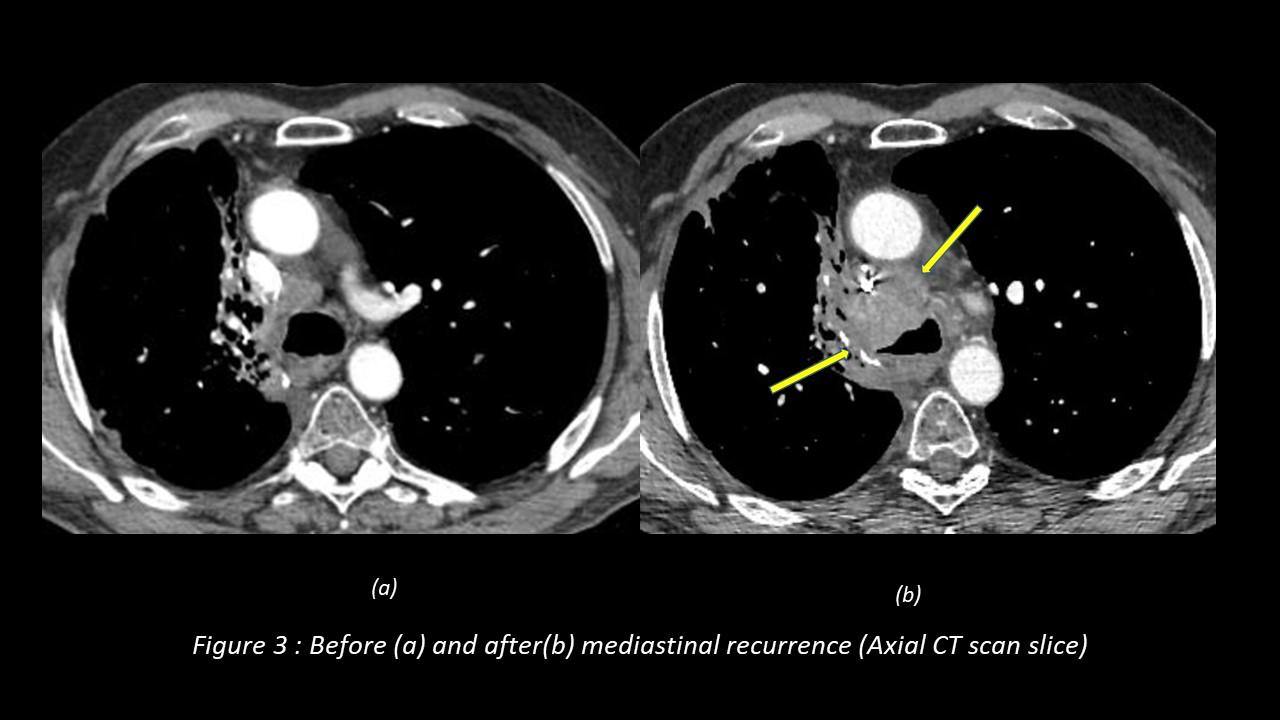
In 2015, a mediastinal lymph node recurrence abruptly worsened his clinical condition (Figure 3), requiring chest radiotherapy and chemotherapy (complicated by pulmonary embolism and aplasia).
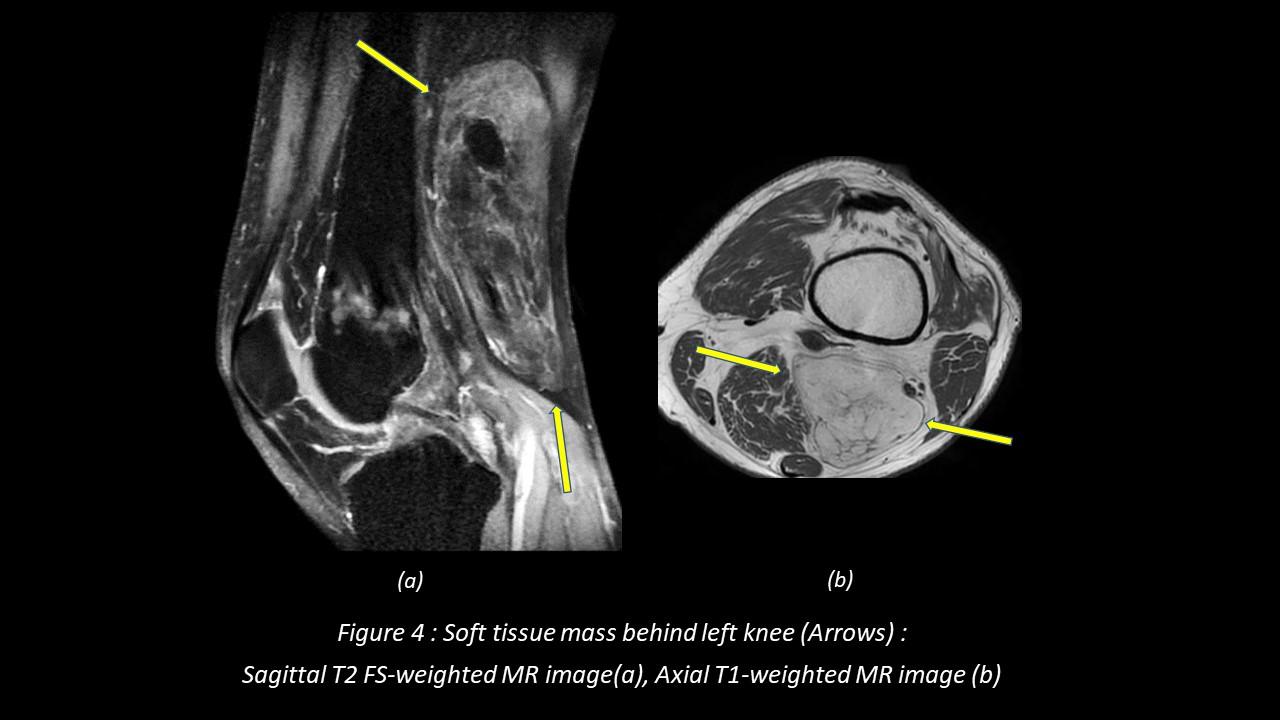
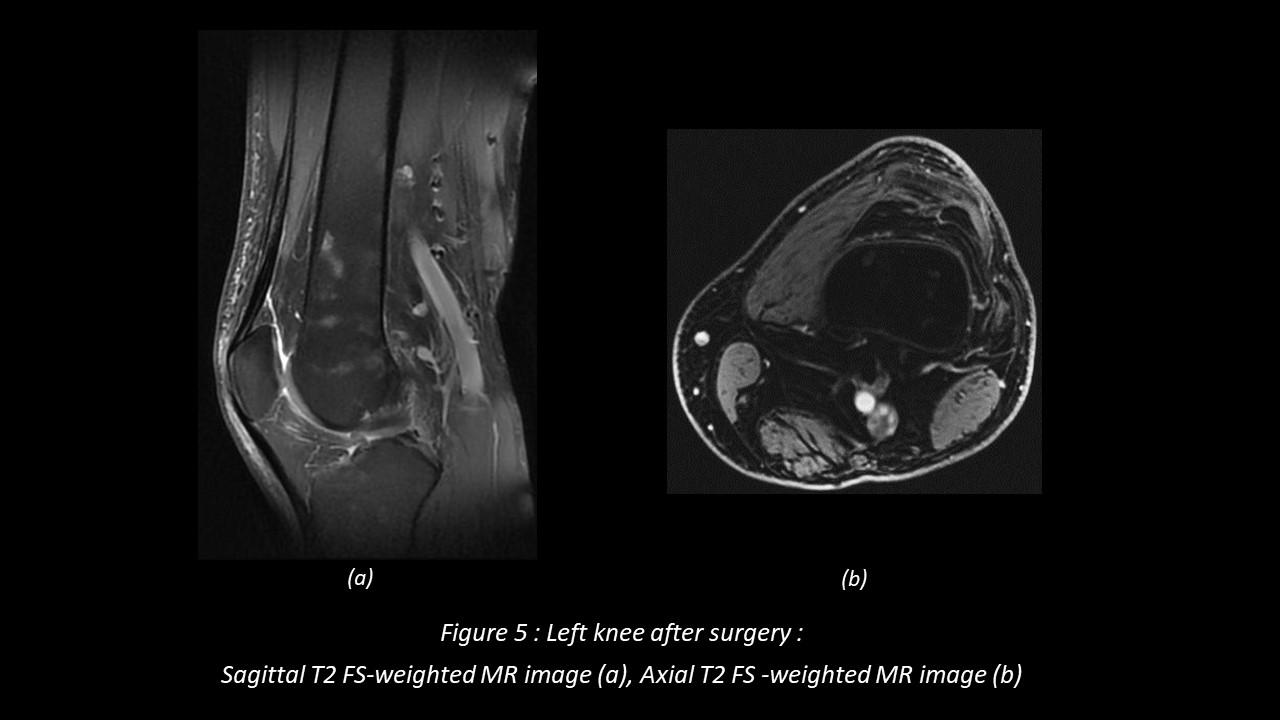
In 2016, a popliteal swelling appeared (behind his left knee) which was revealed after MRI (Figure 4) and biopsy to be a sarcoma (primary lipoma-like). In the same year, a new mediastinal recurrence required the placement of endobronchial prostheses and immunotherapy.
Since 2017, this patient, who has only stopped working (as a real estate agent) episodically during his care pathway, is regularly monitored in imaging by whole-body scanners, MRI of his knee and PET scans / ultrasounds as necessary.
Carrier of 4 histologically different cancers, he is now doing well and has understood that medical imaging has been necessary for the diagnosis and screening of the different tumours of which he is a carrier, the follow-up of treatments and the diagnosis of complications that these treatments induce. He considers himself as a phoenix and is happy to regularly be able to ride his motorcycle.
Radiological Findings
Cigarette smoking is a major risk factor of urothelial tumours of the kidney and urinary tract (1). Patients most often present with macroscopic haematuria or pain induced by urinary tract blockage (2), which was the case with Mr. R.
Ultrasound, CT and MRI make it possible to approach the precise anatomical study of a malignant tumour (essential before surgery if it is indicated). In this case (figure 1-a), the first CT scan in 2009 showed a 3 centimetre right renal pelvic mass tissue (arrows), completely blocking renal excretion (silent kidney) on Rx-Urography (figure 1-b). In 2017, Left Knee MRI of Mr R. revealed a resectable gross (13 centimetres) soft tissue mass in the popliteal region with adipose and non-adipose tissue (figure 4; figure 5 after surgical resection).
Tumour precise diagnosis (cytopathology) is usually made after tumour biopsy (under CT-guidance in 2014 for Mr R., figure 2-b) or after its removal.
Treatments for cancer pathologies require regular follow-ups in variable imaging depending on the case (scanners, MRI, PET scan, scintigraphy, ultrasound etc …). Repeat examinations and follow-up represent an increasing proportion of imaging examinations (3). Imaging, therefore, has an essential role in the early detection of local (mediastinal adenopathy growing between 2 CT follow-up in 2015 for Mr R.: figure 3) or metastatic recurrences and diagnosis of treatment’s complications.
D.Carrié
French Radiologist, MD.
References
- DE. Sweet and al. Infiltrative Renal Malignancies: Imaging Features, Prognostic Implications, and Mimic RadioGraphics 2021; 41:487–508
- A. Prando and al. Urothelial Cancer of the Renal Pelvicaliceal System: Unusual Imaging Manifestations RadioGraphics 2010; 30:1553–1566
- S.I Lee and al. Does Radiologist Recommendation for Follow-up with the Same Imaging Modality Contribute Substantially to High-Cost Imaging Volume? Radiology: Volume 242: Number 3 — March 2007